Michael Turkovich, MS and Linda van Roosmalen, PhD
University of Pittsburgh
ABSTRACT
The majority of US adults are overweight or obese, and individuals with spinal cord injury tend to have a greater percent of fat mass than non SCI adults. With the majority of people traveling in vehicles overweight or obese; it is necessary to examine the effects of obesity on occupant response in frontal impacts since current motor vehicle safety standards are designed for the 50th percentile male and not obese individuals. Computer simulations were run with a modified anthropomorphic test device (ATD) to examine the effects of obesity on occupant kinematics in frontal impact. Results show that head, chest, and pelvis accelerations increased with increasing Body Mass Index (BMI) of the ATD. Chest deformation and forward head excursion also increased with increased BMI. Further analysis is needed to fully describe obese occupant response in order to improve obese occupant safety.
Key words:
obesity, BMI, MADYMOTM, occupant protection
INTRODUCTION
Sixty four percent of US adults are either overweight or obese, and of the 64% approximately 34.3% are considered obese according to the National Center for Health Statistics [1]. This means that approximately 59 million people are considered obese in the United States [2]. The Rehabilitation Research and Training Center reports that people with disability have an 11.6% higher rate of obesity than able-body adults in the US [3], and adults with spinal cord injury tend to have a significantly greater percent of fat mass than non SCI adults [4].
Several studies have examined the effects of obesity on injury patterns and injury severity, and have reported increased risk of injury for the lower extremities, chest, and head for obese individuals in motor vehicle impacts [5-8]. The findings by Mock et al (2002), led them to suggest that occupant restraint systems, and the interior design of the vehicle may need to be modified to fit a person’s body habitus for optimal safety [7]. Current motor vehicle occupant restraint systems are designed for the 50th percentile male [9], and all the research on wheelchair transportation safety is based on this average male ( 50th percentile)[10]. With the growing number of obese people traveling in motor vehicles, it is important to understand how these people respond in impacts so that occupant protection systems can be designed to fit an individual and provide maximum safety.
Objective
The purpose of this study was to examine the effects of obesity on occupant response in frontal impact using computer simulation.
METHODS
 Equation 1
Equation 1The effects of obesity on occupant response in frontal impacts were examined using the computer simulation software MADYMOTM (TNO ,Delft, Netherlands). MADYMOTM is a computer software program commonly used in the automotive industry, and it has a MADYMOTM Anthropomorphic Test Device (ATD) database, which contains validated computer models of ATDs. The MADYMOTM Hybrid III ATD was modified to represent varying degrees of obesity using MADYMOTM Scaler. MADYMOTM Scaler applies different scaling factors to the segments of the ATD [11]. The segment lengths and masses are scaled using Equation 1.
Where λi is the scaling factor in the i direction, Lt is the target length of the segment, Lr is the reference length, and i varies in the x, y, and z directions [11].
 Content for class "floatpicright" Goes Here
Content for class "floatpicright" Goes HereFour MADYMOTM ATDs were generated based on the World Health Organization’s (WHO) classification of Body Mass Index (BMI). BMI is a method used by the WHO to classify obesity and it takes into account a person’s height and weight. BMI is calculated using Equation 2.
Where weight is measured in kilograms (kg) and height is measured in meters (m) [12].
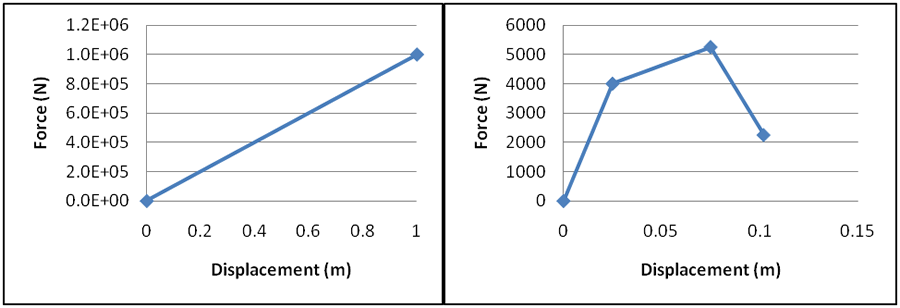 Figure 1. Force-displacement curves for the standard MADYMOTM ATD abdomen (Left) and the abdomen response reported by Hardy et al. 2001 (Right).
Figure 1. Force-displacement curves for the standard MADYMOTM ATD abdomen (Left) and the abdomen response reported by Hardy et al. 2001 (Right).The ATDs generated included a 50th percentile male Hybrid III ATD (BMI = 24), an overweight ATD (BMI=28), an obese ATD (BMI=30) and an obese class II ATD (BMI=35). Since the abdomen of the Hybrid III MADYMOTM ATD does not have a biofidelic response[13], and it has been suggested that the lap belt-obese abdomen interaction is different in the obese population [5, 14], a new material property was assigned to the modified ATDs in the MADYMOTM program. The abdomen was given force-deformation characteristics based on the human cadaver abdomen response corridor for dynamic seatbelt loading generated by Hardy et al. 2001[15]. Figure 1 shows the abdomen force-deflection curves used in the standard MADYMOTM ATD and those reported by Hardy et al 2001.
A frontal impact acceleration pulse of 20g/30mph was applied to all the Modified MAYDMOTM ATDs which were positioned in a generic car seat and restrained by a standard 3 point occupant restraint system. Head acceleration, chest acceleration, pelvis acceleration, head excursion, knee excursion, and chest deformation were recorded for each simulation. Accelerations were measured in units of g. Two dimensional head and knee trajectories were measured in the fore/aft and vertical directions. Chest deformation was defined as the relative displacement of the ATD sternum with respect to the ATD thoracic spine.
RESULTS
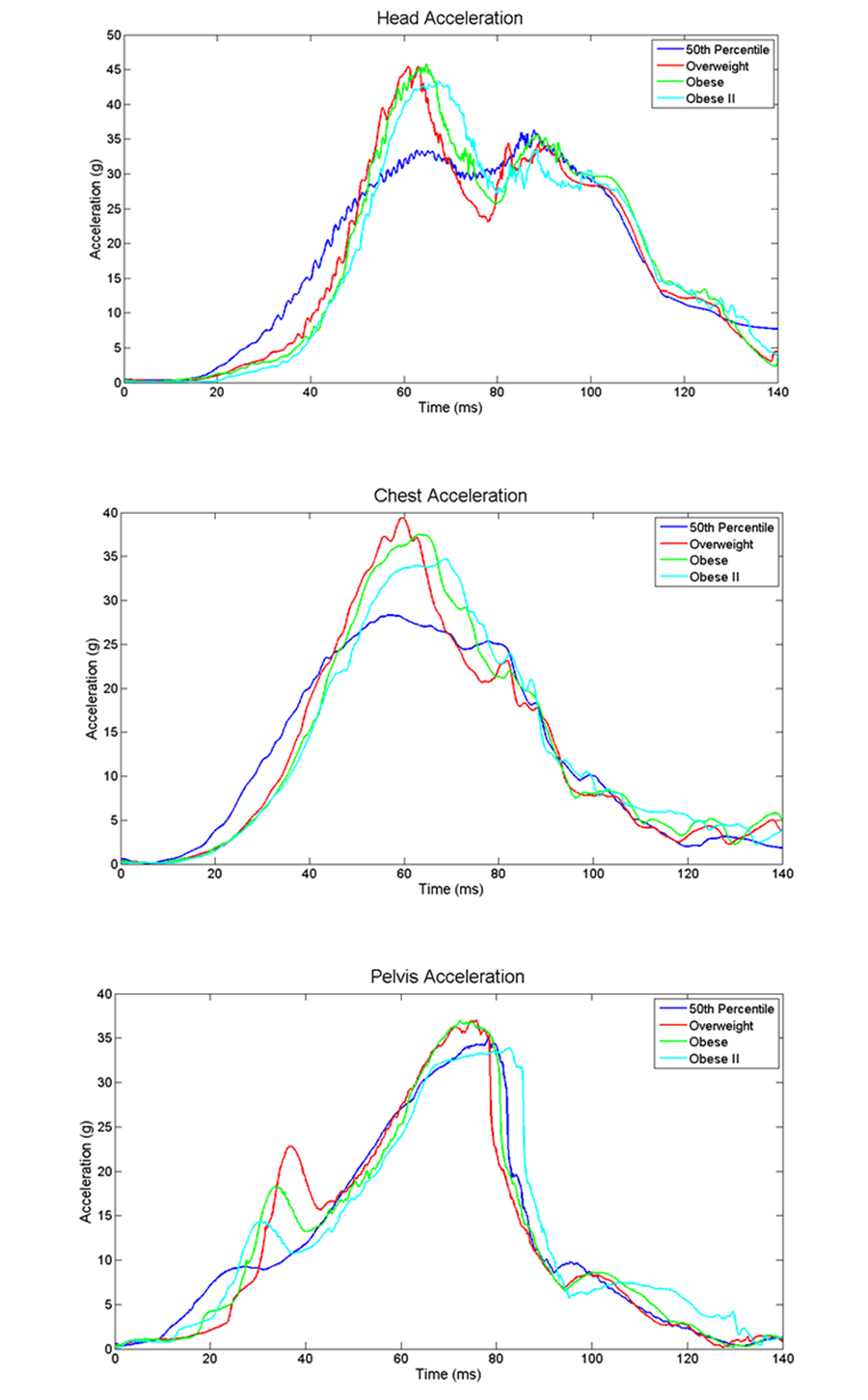 Figure 2. Acceleration plots of ATD head (Top), chest (Middle), and pelvis (Bottom).
Figure 2. Acceleration plots of ATD head (Top), chest (Middle), and pelvis (Bottom). The results of the simulations are presented in Figures 2 and 3. Figure 2 shows that the 50th percentile ATD experiences a lower head, chest, and pelvis acceleration than the modified BMI trials. The increase in BMI causes an earlier peak in head acceleration at approximately 60 ms. There was a slight increase in overweight and obese peak pelvis acceleration but the obese II peak pelvis acceleration was very close to that of the 50th percentile ATD pelvis acceleration.
Figure 3 shows the results for chest deformation and the head and knee trajectories. As BMI increased so did chest deformation. Head excursion in the forward (horizontal) direction increases as BMI is increased, but the head excursion in the vertical direction decreases as BMI is increased. Across BMI scenarios, the knee excursion varies as the BMI increases with a smaller amount of overall knee excursion for the overweight trial compared to the 50th percentile ATD, and increasing excursion for the obese and obese II trials compared to the overweight trial.
DISCUSSION
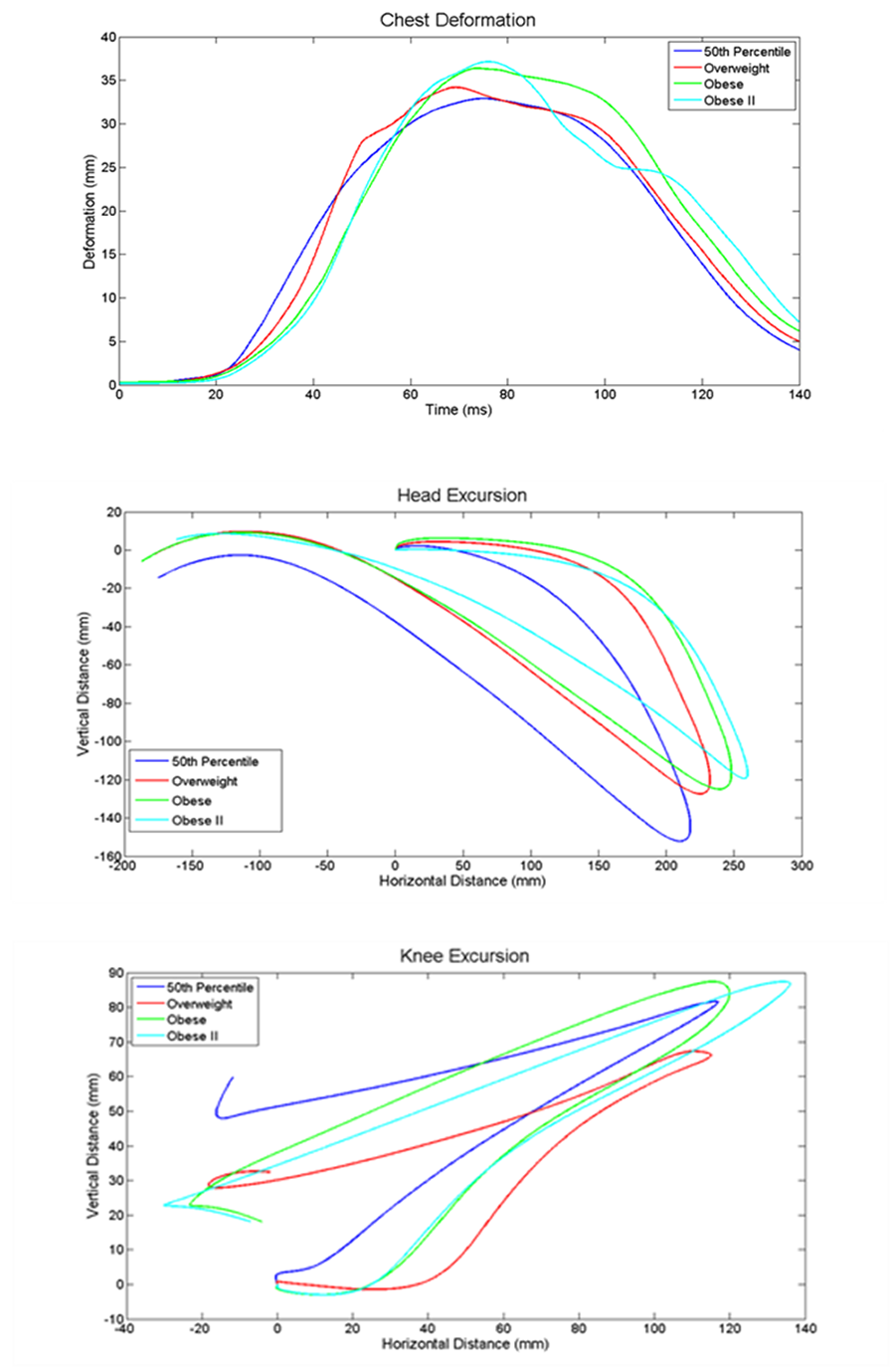 Figure 3. ATD chest deformation (Top), head trajectory (Middle), and knee trajectory (Bottom).
Figure 3. ATD chest deformation (Top), head trajectory (Middle), and knee trajectory (Bottom).Computer simulations were performed to examine the effect of increasing BMI on occupant kinematics in frontal impact. The results show that increasing BMI increases the peak acceleration of the head, chest, and pelvis. The timing of the peak head, chest, and pelvis acceleration was similar for all BMI trials. The increased chest acceleration and increased chest deformation could explain why Cormier 2008 reported that obese occupants have an increased risk of thoracic injury when compared to non-obese occupants in frontal impacts [8].
The peak obese II pelvis acceleration was similar to the 50th percentile peak acceleration. This was unexpected as the other two obesity trials had higher peak accelerations compared to the 50th percentile acceleration. Further analysis revealed that this was due to the modified abdomen. In the obese II trial, the deformation of the abdomen was greater due to the increased mass of the ATD. This resulted in more movement of the ATD pelvis and thus a slightly reduced pelvic acceleration. Further studies on the mechanical response of the obese human abdomen are necessary to understand this phenomenon.
The head trajectory shows that increasing BMI causes an increase in forward movement of the ATD head. This is most likely due to the fact that there is an increased mass being accelerated forward during the impact. This could also explain why obese occupants are more likely to have traumatic brain injury in frontal impacts, as increased forward head excursion increases the likelihood of contact with the interior of the vehicle [16]. However there was also a decrease in the vertical movement of the ATD head. This is most likely due the changes in body dimensions of obese people. The movement of the head is governed by a complex interaction of the pelvis, chest, and neck, all of which may alter as BMI increases.
Knee excursion in the forward and increased in the obese and obese II trials. This was most likely due to the increased mass of the occupant being accelerated forward. It could also explain the increased incidence of lower extremity injuries to obese occupants [6]. There was very little difference in the overweight forward knee excursion and the 50th percentile forward knee excursion, and the overweight trial showed less vertical knee excursion that the other three trials. It is not clear why this occurred and more research is needed to explain results of the overweight knee excursion.
Limitations
It is important to note that this is a preliminary study and therefore more research is needed to fully describe the effects of obesity on occupant kinematics in frontal impacts. While ATDs are the best tool available to examine impact conditions, the MADYMOTM ATD does not fully represent human response or obese human response in frontal impacts. The modification of the MADYMOTM ATD abdomen is a starting point but there is no information on the obese abdominal response in frontal impacts. This limitation is currently being investigated further. Finally the scaling of the MADYMOTM ATD provides an obese ATD but it does not necessarily represent the common mass distribution of obese people.
CONCLUSION
This preliminary study of the effects of obesity on occupant kinematics shows that increased BMI causes increased MADYMOTM ATD head, chest and pelvis accelerations. BMI also causes increase chest deformation and forward head excursion. The increases in these parameters suggest that obese individuals may be at a greater risk of injury in motor vehicle impacts. In order to provide improved occupant protection to obese individuals, safety systems need to be designed to “fit” a person’s body dimensions and withstand the forces associated with frontal impact. This is especially important given the trends of increased obesity in US adults and people with disabilities. Further research is necessary to accurately describe the effects of obesity on occupants in frontal impacts.
REFERENCES
- National Center for Health Statistics, Health, United States. 2006.
- Center for Disease Control. Obesity in US Adults: 2007.
- Rehabilitation Research and Training Center on Disability Statistics and Demographics, Annual Compendium of Disability Statistics Compendium: 2009 Rehabilitation Research and Training Center on Disability Demographics and Statistics, Hunter and College, Editors. 2009.
- Buchholz, A. and Bugaresti, J., A review of body mass index and waist circumference as markers of obesity and coronary heart disease risk in persons with chronic spinal cord injury. Spinal Cord, 2005. 43: p. 513-518.
- Arbabi, S., Wahl, W.L., Hemmila, M.R., Kohoyda-Inglis, C., Taheri, P.A., and Wang, S.C., The Cushion Effect. The Journal of Trauma Injury, Infection, and Critical Care, 2003. 54: p. 1090-1093.
- Boulanger, B.R., Milzman, D., Mitchell, K., and Rodriguez, A., Body habitus as a predictor of injury pattern after blunt trauma. The Journal of Trauma Injury, Infection, and Critical Care, 1992. 33: p. 228-232.
- Mock, C.N., Grossman, D.C., Kaufman, R.P., Mack, C.D., and Rivara, F.P., The relationship between body weight and risk of death and serious injury in motor vehicle crashes. Accident Analysis and Prevention, 2002. 34: p. 221-228.
- Cormier, J.M., The influence of body mass index on thoracic injuries in frontal impacts. Accident Analysis and Prevention, 2008. 40: p. 610-615.
- National Traffic and Highway Safety Administration, FMVSS 208, U.D.o. Transportation, Editor.
- American National Standards Organization (ANSI), ANSI/RESNA WC-19: Wheelchairs used as seats in motor vehicles. 2000, American National Standards Institute/Rehabilitation Engineering Society of North America (ANSI/RESNA) Wheelchair Standards: Arlington, Va.
- TNO, Madymo Utilities Manual Release 6.3.2. 2006.
- World Health Organization, Global Database on Body Mass Index. 2009.
- TNO, Madymo Model Manual Release 6.3.2. 2006.
- Wang, S.C., Bednarski, B., Patel, S., Yan, A., Kohoyda-Inglis, C., Kennedy, T., Link, E., Rowe, S., Sochor, M., and Arbabi, S. Increased Depth of Subcutaneous Fat is Protective against Abdominal Injuries in Motor Vehicle Collisions. in 47th Proceedings of the Association for the Advancement of Automotive Medicine. 2003.
- Hardy, W.N. and Schneider, L.W., Abdominal Impact Response to Rigid-Bar, Seatbelt, and Airbag Loading. Stapp Car Crash Journal, 2001. 45: p. 1-32.
- Tagliaferri, F., Compagnone, C., Yoganandan, N., and Gennarelli, T.A., Traumatic Brain Injury After Frontal Crashes: Relationship with Body Mass Index. The Journal of Trauma Injury, Infection, and Critical Care, 2009. 66: p. 727-729.
Acknowledgments
This study was partially supported by the Dept. of Education, NIDRR and the RERC on WTS grant #H133E060064.
Contact:
Michael Turkovich, 6425 Penn Ave. Suite 401, Pittsburgh, Pa 15206. Phone #: 412-624-6433
Word Version PDF Version